名家视点丨宓余强教授:NAFLD相关肝癌研究进展
—— 作者: 时间:2024-02-12
阅读数:
70
编者按
非酒精性脂肪性肝病(NAFLD)和肝细胞癌(HCC)的疾病负担沉重,近20年NAFLD相关HCC已成为全球日益严重的公共卫生问题。在慢性病毒性肝炎高发的亚洲,同样面临NAFLD及其相关HCC发病率的不断升高。为此,本刊特邀请天津市第二人民医院宓余强教授撰文,针对当前HCC病因的变化趋势及NAFLD相关HCC的流行率、NAFLD相关HCC的危险因素、筛查和治疗方法进行综述,旨在为改善NAFLD的预后和减少其HCC发病风险的临床研究提供指导。
NAFLD相关HCC流行病学及自然史
非酒精性脂肪性肝病(NAFLD)是世界上最常见的慢性肝病[1],组织学特点为肝脏脂肪变性≥5%[2]。疾病谱包括非酒精性肝脂肪变、非酒精性脂肪性肝炎(NASH)、肝硬化和肝细胞癌(HCC),亚洲患病率高达约30%[1,3]。
自2000年以来,NAFLD患者的肝细胞癌(HCC)发病率也在全球范围内大幅增加,NAFLD正在成为HCC的主要原因[4,5]。根据2019年全球疾病负担数据显示,NAFLD相关HCC的发病率占总体HCC的6.8%,并预计将持续增加[6]。NAFLD人群的HCC年发病率为0.021%,NAFLD相关肝硬化患者HCC的年发病率为0.5%~2.6%[7]。估计每100例NAFLD中约有1或2例发展为HCC[8, 9]。
在美国、法国和英国,NAFLD已经成为增长最快的HCC病因。在全球范围内,NAFLD相关HCC的发病率也可能随之增加[10]。预计到2030年,NAFLD相关HCC的发病率将急剧上升,中国、法国和美国将分别比2016年增加82%、117%和122%[10]。
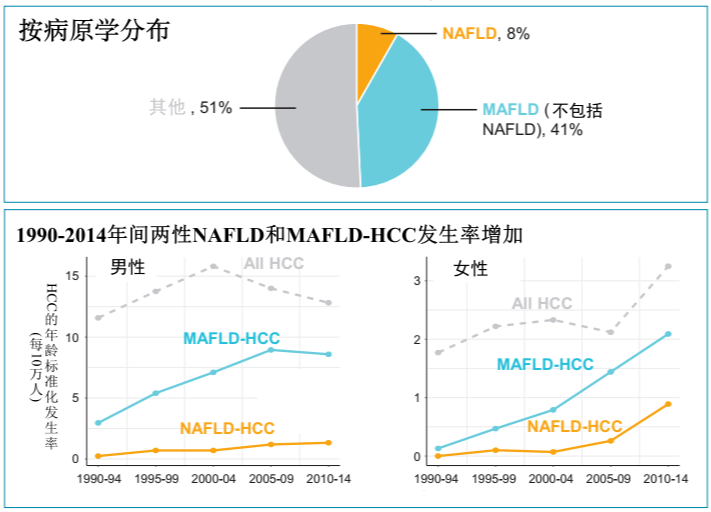
图1. 瑞士日内瓦920例HCC患者的人群研究(1990-2014)
NAFLD相关HCC危险因素
01
糖尿病
NAFLD合并糖尿病(DM)的患者进展为HCC的风险很高。在一项对85963例NAFLD合并DM患者长达10年的随访中发现,DM合并NAFLD患者发生HCC的风险比非DM患者高24%[11]。DM增加NAFLD相关HCC发生风险潜在机制可能是胰岛素抵抗引起代谢紊乱,造成脂肪肝和肝纤维化,最终导致肝硬化、HCC的发生[12]。
02
肥胖
多项研究均表明,肥胖会增加NAFLD相关HCC的发生风险。一项队列研究表明,在BMI高于35.0的男性中,HCC死亡的RR比体重正常的男性增加了近5倍(RR=4.52)[13]。当糖尿病、肥胖、动脉高血压和血脂异常相伴行时,NAFLD相关HCC发生的风险将进一步增加。
03
年龄和性别
在一项覆盖近30万NAFLD患者的大型队列研究中,年龄≥65岁是HCC发生的独立危险因素[7]。多数研究表明,NAFLD相关HCC患者通常是老年患者[14-16],HCC在男性中的发病率高于女性,分别为0.022%和0.004%。而有几项研究表明,男性发生HCC的风险是女性的4倍[15,17,18]。
04
遗传学和种族
研究显示, patatin样磷脂酶结构域蛋白3(PNPLA3)的基因多态性与HCC发生风险的增加密切相关[19]。PNPLA3使NAFLD相关肝硬化患者发生HCC的风险增加了1.67倍[20]。此外,西班牙裔NAFLD患者的HCC年发生率(0.029%)高于白人(0.021%)和非裔美国人(0.012%)[10]。
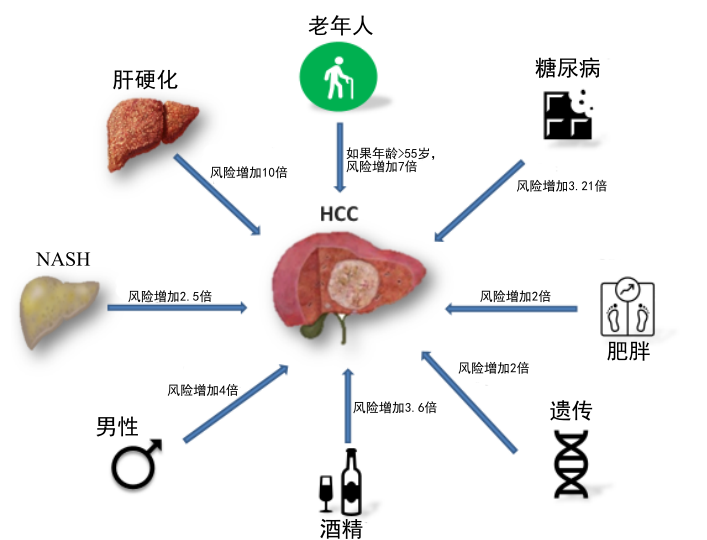
图2. NAFLD患者发生HCC的主要危险因素
NAFLD相关HCC发病机制
01
炎症和细胞因子
NAFLD患者往往有超重或肥胖,超重或肥胖能够促进各种细胞因子释放,细胞因子可促进肝脏微环境的免疫耐受和炎症,激活JAK通路导致细胞增殖,同时肿瘤坏死因子-α(TNF-α)和白细胞介素-6(IL-6)可通过激活STAT3通路促进细胞增殖,进而促进HCC的发生。NAFLD患者胰岛素样生长因子(IGF)水平增加,IGF能抑制细胞凋亡和刺激细胞分裂,在肿瘤的浸润转移中发挥促进作用[10,21,22]。
02
氧化应激
NAFLD特点是肝脏脂肪堆积增加和慢性炎症,导致活性氧(ROS)水平过高,线粒体功能障碍和内质网应激。ROS的增加导致氧化应激和肝损伤,从而导致NAFLD的进展,这与HCC密切相关。游离脂肪酸亚油酸可破坏线粒体功能,介导ROS相关的CD4+T淋巴细胞选择性死亡,降低免疫监视[23, 24],IgA+细胞在NASH中积聚可抑制CD8+T细胞并加速HCC的发生[25]。
03
成纤维细胞生长因子(FGF)信号
FGFs和成纤维细胞生长因子受体(FGFRs)可以促进和驱动NAFLD向NASH、HCC发展,并在某些情况下具有致癌潜力[28]。特别是FGF19、FGF21和FGF23在生理上具有调节胆汁酸和葡萄糖等内分泌功能,并调节空腹反应、脂质代谢等[29-33]。由于这些代谢途径的失调被认为是导致NAFLD、NASH、肝纤维化和HCC的慢性肝脏疾病的关键特征,FGFs和FGFR可能是诊断、监测和治疗这些疾病的新靶点。
04
肠道菌群
在NAFLD中,保护性肠道细菌的减少和法尼醇X受体(FXR)信号的失调增加了肠道通透性和肝脏炎症,导致肝脏炎症和纤维化,加速了HCC的发生[26]。在NAFLD相关HCC患者中,微生物群与血液中较高水平的IL-8、IL-13、CCL-3、CCL-4和CCL-5以及与活化的循环单核细胞相关[27]。这些与HCC相关的微生物群变化加剧炎症并促进HCC的发展。
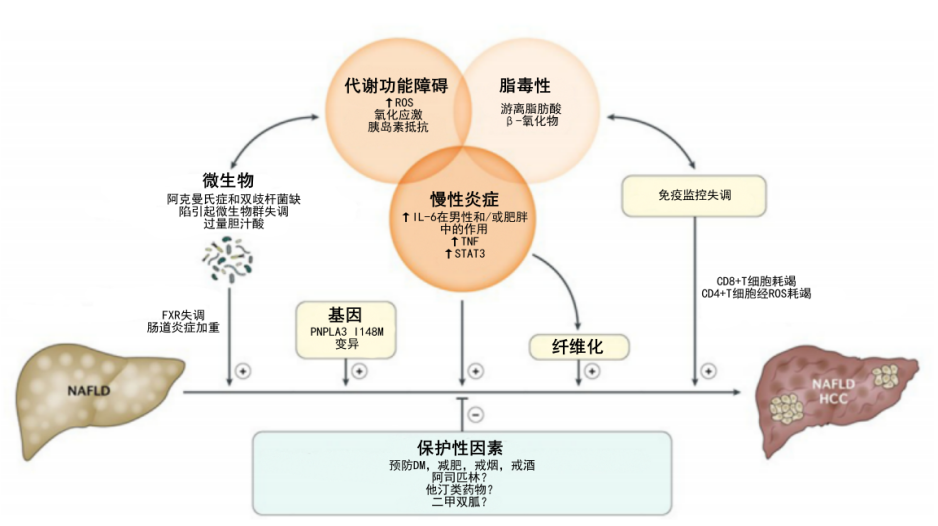
图3. NAFLD相关HCC的发病机制及预防
NAFLD相关HCC的预测及筛查管理
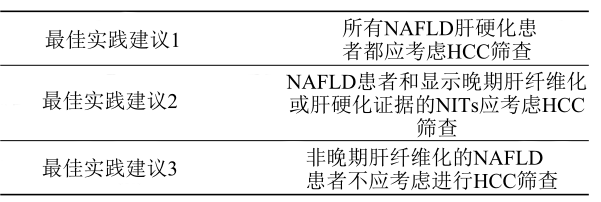
临床实践中应充分利用无创诊断方法(无创性血清学评分的应用、彩色多普勒超声、Fibroscan或者Fibrotouch、血清肿瘤标志物检测等)进行早期筛查,若发现预警信号再进一步行CT或者MRI检查[34]。美国胃肠病学会(AGA)临床实践指南建议对于提示存在晚期纤维化(F3)或肝硬化的患者,应考虑血液检查和影像学检查结合,进行HCC筛查[35]。对于肝硬化、NITs诊断疑似晚期纤维化以及糖尿病患者,应每半年进行一次超声检查,并检测肿瘤标志物如PIVKA-II、AFP、AFP-L3和GPC-3[36]。
流行病学和遗传学研究表明,遗传模式可以解释一些NAFLD表型和进展风险的变异性。遗传因素对HCC易感性有影响,且家族聚集性强[37]。目前,至少有三种常见的基因变异与NAFLD有密切的联系,分别是PNPLA3、TM6SF2和MBOAT7。这些基因的功能揭示了NAFLD发生发展的新途径[38]。
表1. AGA 关于NAFLD相关HCC的监测建议
NAFLD相关HCC的治疗及预后
与非NAFLD相关HCC相比,NAFLD相关HCC常发现较晚,故较少能够接受根治性治疗[39]。然而,一项数据分析表明,除了肝功能受损之外,血清白蛋白水平≥3.7 g/dl的NAFLD相关HCC患者,接受肝切除术或射频消融(RFA)治疗的预后最好[40]。NAFLD相关HCC通过积极治疗是否较非NAFLD相关HCC获得更好的长期生存益处有待进一步证实。
对于NAFLD相关HCC,改变生活方式是目前循证医学已证实预防和延缓NAFLD进展的重要手段[41]。一项覆盖近47万病例的前瞻性调查研究揭示了运动与HCC发展风险之间呈负相关[42]。减重手术可减少肥胖患者NASH-HCC的发生[43]。越来越多的证据表明,糖尿病药物也可能是有效的治疗方法。二甲双胍是一种胰岛素增敏剂,通过激活腺苷酸活化蛋白激酶信号通路来减少HCC的发生。一项大型队列研究发现,二甲双胍可以使HCC风险降低70%[42],与肝硬化患者总体死亡率的下降独立相关[44]。噻唑烷二酮类(TZDs)是另一类能激活PPAR的抗糖尿病药物,PPAR是葡萄糖代谢和胰岛素敏感性的关键调节因子,有证据表明这些药物参与细胞生长抑制、诱导凋亡和防止细胞入侵和抗肿瘤[45,46],可以降低HCC风险。他汀类药物具有抗炎、抗血管生成和抗增殖作用,可有效对抗由炎症驱动所导致的癌症[47],可使HCC发病率降低37%。他汀类药物还可以改善NAFLD患者血脂异常、降低心血管疾病风险、降低NAFLD相关的死亡率[47,48]。阿司匹林能减少T细胞介导的炎症,减缓肝纤维化的发展,并能减少小鼠模型HCC的形成[49]。阿司匹林摄入与HCC风险降低相关,而且这种作用不受他汀类药物的影响[50]。能有效治疗NASH的药物是否也能降低HCC的相关风险,仍有待观察。
参考文献:
[1] LI J, ZOU B, YEO Y H, et al. Prevalence, incidence, and outcome of non-alcoholic fatty liver disease in Asia, 1999-2019: a systematic review and meta-analysis [J]. Lancet Gastroenterol Hepatol, 2019, 4(5): 389-98.
[2] CHALASANI N, YOUNOSSI Z, LAVINE J E, et al. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases [J]. Hepatology, 2018, 67(1): 328-57.
[3] LE M H, YEO Y H, LI X, et al. 2019 Global NAFLD Prevalence: A Systematic Review and Meta-analysis [J]. Clin Gastroenterol Hepatol, 2022, 20(12): 2809-17 e28.
[4] YOUNES R, BUGIANESI E. Should we undertake surveillance for HCC in patients with NAFLD? [J]. J Hepatol, 2018, 68(2): 326-34.
[5] STINE J G, WENTWORTH B J, ZIMMET A, et al. Systematic review with meta-analysis: risk of hepatocellular carcinoma in non-alcoholic steatohepatitis without cirrhosis compared to other liver diseases [J]. Aliment Pharmacol Ther, 2018, 48(7): 696-703.
[6] LIU Y, ZHENG J, HAO J, et al. Global burden of primary liver cancer by five etiologies and global prediction by 2035 based on global burden of disease study 2019 [J]. Cancer Med, 2022, 11(5): 1310-23.
[7] KANWAL F, KRAMER J R, MAPAKSHI S, et al. Risk of Hepatocellular Cancer in Patients With Non-Alcoholic Fatty Liver Disease [J]. Gastroenterology, 2018, 155(6): 1828-37 e2.
[8] DIEHL A M, DAY C. Cause, Pathogenesis, and Treatment of Nonalcoholic Steatohepatitis [J]. New England Journal of Medicine, 2017, 377(21): 2063-72.
[9] SUMIDA Y, YONEDA M, SEKO Y, et al. Surveillance of Hepatocellular Carcinoma in Nonalcoholic Fatty Liver Disease [J]. Diagnostics (Basel), 2020, 10(8).
[10] HUANG D Q, EL-SERAG H B, LOOMBA R. Global epidemiology of NAFLD-related HCC: trends, predictions, risk factors and prevention [J]. Nat Rev Gastroenterol Hepatol, 2021, 18(4): 223-38.
[11] KRAMER J R, NATARAJAN Y, DAI J, et al. Effect of diabetes medications and glycemic control on risk of hepatocellular cancer in patients with nonalcoholic fatty liver disease [J]. Hepatology, 2022, 75(6): 1420-8.
[12] ASRIH M, JORNAYVAZ F R. Metabolic syndrome and nonalcoholic fatty liver disease: Is insulin resistance the link? [J]. Mol Cell Endocrinol, 2015, 418 Pt 1: 55-65.
[13] CALLE E E, RODRIGUEZ C, WALKER-THURMOND K, et al. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults [J]. N Engl J Med, 2003, 348(17): 1625-38.
[14] MITTAL S, EL-SERAG H B, SADA Y H, et al. Hepatocellular Carcinoma in the Absence of Cirrhosis in United States Veterans is Associated With Nonalcoholic Fatty Liver Disease [J]. Clin Gastroenterol Hepatol, 2016, 14(1): 124-31 e1.
[15] PISCAGLIA F, SVEGLIATI‐BARONI G, BARCHETTI A, et al. Clinical patterns of hepatocellular carcinoma in nonalcoholic fatty liver disease: A multicenter prospective study [J]. Hepatology, 2016, 63(3): 827-38.
[16] PERUMPAIL R B, WONG R J, AHMED A, et al. Hepatocellular Carcinoma in the Setting of Non-cirrhotic Nonalcoholic Fatty Liver Disease and the Metabolic Syndrome: US Experience [J]. Dig Dis Sci, 2015, 60(10): 3142-8.
[17] EUROPEAN ASSOCIATION FOR THE STUDY OF THE LIVER. ELECTRONIC ADDRESS E E E, EUROPEAN ASSOCIATION FOR THE STUDY OF THE L. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma [J]. J Hepatol, 2018, 69(1): 182-236.
[18] VILAR-GOMEZ E, CALZADILLA-BERTOT L, WAI-SUN WONG V, et al. Fibrosis Severity as a Determinant of Cause-Specific Mortality in Patients With Advanced Nonalcoholic Fatty Liver Disease: A Multi-National Cohort Study [J]. Gastroenterology, 2018, 155(2): 443-57 e17.
[19] STENDER S, LOOMBA R. PNPLA3 Genotype and Risk of Liver and All‐Cause Mortality [J]. Hepatology, 2020, 71(3): 777-9.
[20] SINGAL A G, MANJUNATH H, YOPP A C, et al. The Effect of PNPLA3 on Fibrosis Progression and Development of Hepatocellular Carcinoma: A Meta-analysis [J]. Official journal of the American College of Gastroenterology | ACG, 2014, 109(3): 325-34.
[21] YOUNOSSI Z, STEPANOVA M, ONG J P, et al. Nonalcoholic Steatohepatitis Is the Fastest Growing Cause of Hepatocellular Carcinoma in Liver Transplant Candidates [J]. Clin Gastroenterol Hepatol, 2019, 17(4): 748-55 e3.
[22] PARK E J, LEE J H, YU G Y, et al. Dietary and genetic obesity promote liver inflammation and tumorigenesis by enhancing IL-6 and TNF expression [J]. Cell, 2010, 140(2): 197-208.
[23] AMORIM R, MAGALHAES C C, BORGES F, et al. From Non-Alcoholic Fatty Liver to Hepatocellular Carcinoma: A Story of (Mal)Adapted Mitochondria [J]. Biology (Basel), 2023, 12(4).
[24] MA C, KESARWALA A H, EGGERT T, et al. NAFLD causes selective CD4(+) T lymphocyte loss and promotes hepatocarcinogenesis [J]. Nature, 2016, 531(7593): 253-7.
[25] SHALAPOUR S, LIN X J, BASTIAN I N, et al. Inflammation-induced IgA+ cells dismantle anti-liver cancer immunity [J]. Nature, 2017, 551(7680): 340-5.
[26] SHARPTON S R, AJMERA V, LOOMBA R. Emerging Role of the Gut Microbiome in Nonalcoholic Fatty Liver Disease: From Composition to Function [J]. Clin Gastroenterol Hepatol, 2019, 17(2): 296-306.
[27] PONZIANI F R, BHOORI S, CASTELLI C, et al. Hepatocellular Carcinoma Is Associated With Gut Microbiota Profile and Inflammation in Nonalcoholic Fatty Liver Disease [J]. Hepatology, 2019, 69(1): 107-20.
[28] BEENKEN A, MOHAMMADI M. The FGF family: biology, pathophysiology and therapy [J]. Nat Rev Drug Discov, 2009, 8(3): 235-53.
[29] FU L, JOHN L M, ADAMS S H, et al. Fibroblast growth factor 19 increases metabolic rate and reverses dietary and leptin-deficient diabetes [J]. Endocrinology, 2004, 145(6): 2594-603.
[30] KHARITONENKOV A. FGFs and metabolism [J]. Curr Opin Pharmacol, 2009, 9(6): 805-10.
[31] LUNDASEN T, GALMAN C, ANGELIN B, et al. Circulating intestinal fibroblast growth factor 19 has a pronounced diurnal variation and modulates hepatic bile acid synthesis in man [J]. J Intern Med, 2006, 260(6): 530-6.
[32] ZHANG X, YEUNG D C, KARPISEK M, et al. Serum FGF21 levels are increased in obesity and are independently associated with the metabolic syndrome in humans [J]. Diabetes, 2008, 57(5): 1246-53.
[33] XU J, LLOYD D J, HALE C, et al. Fibroblast growth factor 21 reverses hepatic steatosis, increases energy expenditure, and improves insulin sensitivity in diet-induced obese mice [J]. Diabetes, 2009, 58(1): 250-9.
[34] POYNARD T, MUNTEANU M, LUCKINA E, et al. Liver fibrosis evaluation using real-time shear wave elastography: applicability and diagnostic performance using methods without a gold standard [J]. J Hepatol, 2013, 58(5): 928-35.
[35] LOOMBA R, LIM J K, PATTON H, et al. AGA Clinical Practice Update on Screening and Surveillance for Hepatocellular Carcinoma in Patients With Nonalcoholic Fatty Liver Disease: Expert Review [J]. Gastroenterology, 2020, 158(6): 1822-30.
[36] CAVIGLIA G P, ARMANDI A, ROSSO C, et al. Biomarkers of Oncogenesis, Adipose Tissue Dysfunction and Systemic Inflammation for the Detection of Hepatocellular Carcinoma in Patients with Nonalcoholic Fatty Liver Disease [J]. Cancers (Basel), 2021, 13(10).
[37] TURATI F, EDEFONTI V, TALAMINI R, et al. Family history of liver cancer and hepatocellular carcinoma [J]. Hepatology, 2012, 55(5): 1416-25.
[38] PENNISI G, CELSA C, GIAMMANCO A, et al. The Burden of Hepatocellular Carcinoma in Non-Alcoholic Fatty Liver Disease: Screening Issue and Future Perspectives [J]. Int J Mol Sci, 2019, 20(22).
[39] FOERSTER F, GAIRING S J, MULLER L, et al. NAFLD-driven HCC: Safety and efficacy of current and emerging treatment options [J]. J Hepatol, 2022, 76(2): 446-57.
[40] KAWAGUCHI T, TOKUSHIGE K, HYOGO H, et al. A Data Mining-based Prognostic Algorithm for NAFLD-related Hepatoma Patients: A Nationwide Study by the Japan Study Group of NAFLD [J]. Sci Rep, 2018, 8(1): 10434.
[41] KOGISO T, TOKUSHIGE K. The Current View of Nonalcoholic Fatty Liver Disease-Related Hepatocellular Carcinoma [J]. Cancers (Basel), 2021, 13(3).
[42] ZHANG Z-J, ZHENG Z-J, SHI R, et al. Metformin for Liver Cancer Prevention in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis [J]. The Journal of Clinical Endocrinology & Metabolism, 2012, 97(7): 2347-53.
[43] KWAK M, MEHAFFEY J H, HAWKINS R B, et al. Bariatric surgery is associated with reduction in non-alcoholic steatohepatitis and hepatocellular carcinoma: A propensity matched analysis [J]. Am J Surg, 2020, 219(3): 504-7.
[44] KAPLAN D E, SERPER M, JOHN B V, et al. Effects of metformin exposure on survival in a large national cohort of patients with diabetes and cirrhosis [J]. Clinical Gastroenterology and Hepatology, 2021, 19(10): 2148-60. e14.
[45] CHO Y Y, YU S J, LEE H W, et al. Clinical Characteristics of Long-Term Survivors After Sorafenib Treatment for Unresectable Hepatocellular Carcinoma: A Korean National Multicenter Retrospective Cohort Study [J]. J Hepatocell Carcinoma, 2021, 8: 613-23.
[46] CHANG C-H, LIN J-W, WU L-C, et al. Association of thiazolidinediones with liver cancer and colorectal cancer in type 2 diabetes mellitus [J]. Hepatology, 2012, 55(5): 1462-72.
[47] PASTORI D, PANI A, DI ROCCO A, et al. Statin liver safety in non-alcoholic fatty liver disease: A systematic review and metanalysis [J]. British Journal of Clinical Pharmacology, 2022, 88(2): 441-51.
[48] REINER Z. Statins in the primary prevention of cardiovascular disease [J]. Nat Rev Cardiol, 2013, 10(8): 453-64.
[49] SITIA G, AIOLFI R, DI LUCIA P, et al. Antiplatelet therapy prevents hepatocellular carcinoma and improves survival in a mouse model of chronic hepatitis B [J]. Proceedings of the National Academy of Sciences, 2012, 109(32): E2165-E72.
[50] LEE T Y, HSU Y C, HO H J, et al. Daily aspirin associated with a reduced risk of hepatocellular carcinoma in patients with non-alcoholic fatty liver disease: a population-based cohort study [J]. EClinicalMedicine, 2023, 61: 102065.
声明:本文仅供医疗卫生专业人士了解最新医药资讯参考使用,不代表本平台观点。该信息不能以任何方式取代专业的医疗指导,也不应被视为诊疗建议,如果该信息被用于资讯以外的目的,本站及作者不承担相关责任。
标签:
访谈
专家访谈
非酒精性脂肪性肝病
发表评论
全部评论
